


RELATED PRODUCTS NOT AVAILABLE
true
Support
Becton, Dickinson and Company
0124-4124300
bd_india@bd.com
Contact Us
Thank you for contacting our sales team!
A sales representive will get in touch with you shortly.
Address
6th Floor Signature Tower - B, South City I, NH 8 Gurgaon, 122001, Haryana
Covera™ Vascular Covered Stent
The ONLY Covered Stent Indicated for AV Grafts and Native AV Fistula***

- Overview
- Clinical Experience
- Products & Accessories
- EIFU & Resources
The covered stent Tailor-Made for AV patients
The Covera™ Vascular Covered Stent builds upon proven technologies from the category leader in AV access. This covered stent platform is designed to balance the flexibility and strength required to address challenging lesions from the terminal cephalic arch, to the basilic swingpoint segments, to the AV graft venous anastomosis. Flared and straight configurations allow for precise sizing and adaptation to the vessel wall, while an easy-to-use thumbwheel delivery system with two speed options provides placement control.
The Covera™ Vascular Covered Stent delivered effective results in two separate clinical trials, one for patients dialyzing with AV grafts and one for patients dialyzing with AV fistulas.1

For radial strength and flexibility
Unique, flexible base stent architecture designed to conform to native vessel in challenging AV anatomy.
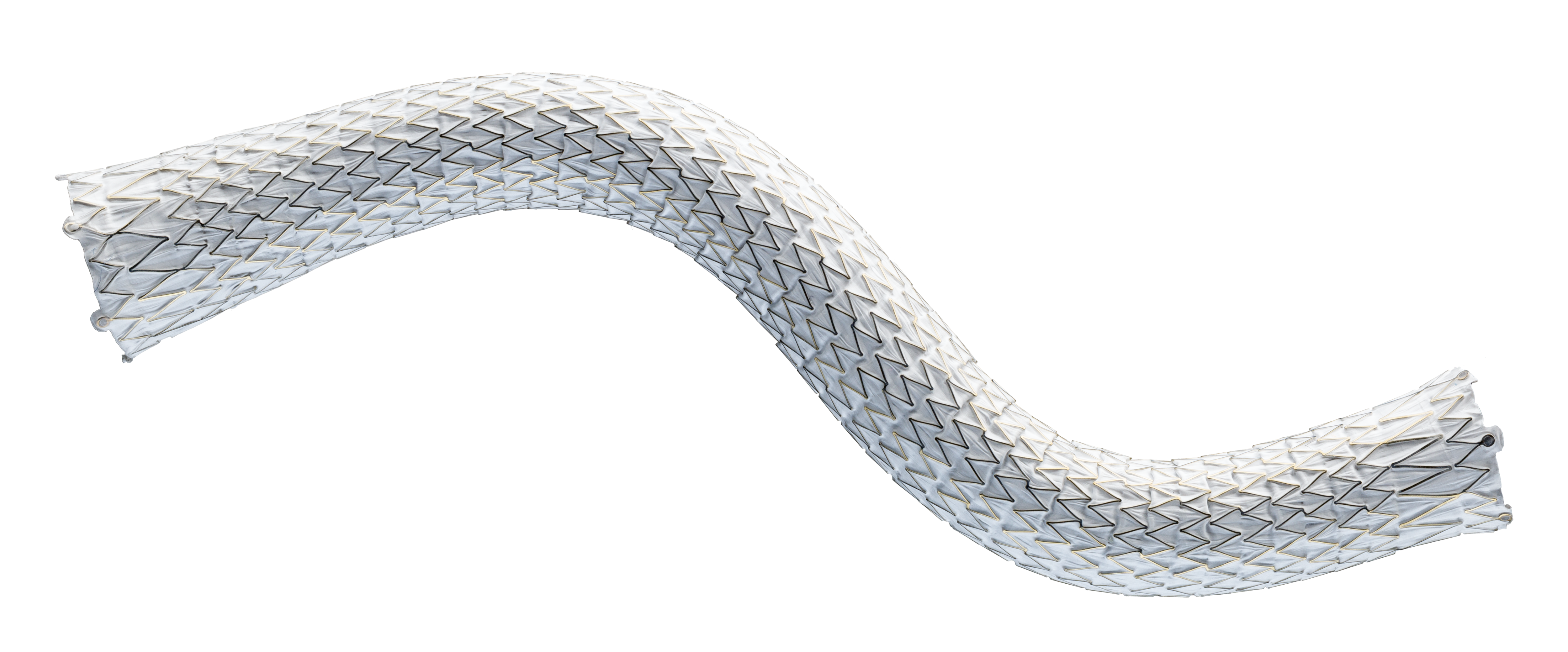
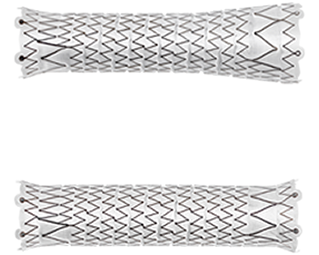
Straight and Flared configurations for optimized hemodynamic flow at the venous anastomosis
- Straight configurations are intended for use in anatomies where the diameter of the outflow vessel is equal to or smaller than that of the inflow vessel
- Flared configuration is intended for use in anatomies where the diameter of the outflow vessel is larger than that of the inflow vessel

Atraumatic tip designed for ease of insertion and removal at the access site
Facilitates accurate placement control
Intuitive triaxial delivery system designed for precise placement and to faciliate optimal lesion coverage


*** In the U.S. as of Jan. 2023
1 Dolmatch B, Waheed U, Balamuthusamy S, Hoggard J, Settlage R; AVeVA Trial Investigators. Prospective, Multicenter Clinical Study of the Covera Vascular Covered Stent in the Treatment of Stenosis at the Graft-Vein Anastomosis of Dysfunctional Hemodialysis Access Grafts. J Vasc Interv Radiol. 2022;33(5):479-488.e3. doi:10.1016/j. jvir.2022.02.008. AVeNEW Clinical Studies data on file. At 6 months in AVeVA target lesion primary patency (TLPP) was 70.3% (proportional analysis). At 6 months in AVeNEW, TLPP was 78.7% for Covera™ Vascular Covered Stent vs. 47.9% for PTA alone, P < .001. 130 of the 142 (91.5%) subjects randomized to the Covera™ Vascular Stent group and 123 of the 138 (89.1%) randomized to PTA completed their 6-month follow-up. TLPP defined as the interval following the index intervention until the next clinically-driven reintervention at or adjacent to the original treatment site or until the extremity was abandoned for permanent access. In AVeNEW, TLPP at 6 Months – Subgroup Analysis is provided as observational data without P values. In AVeNEW, patients who received the Covera™ Vascular Covered Stent had 103 reinterventions involving a new lesion compared to 72 reinterventions in the PTA only group at 24 months. At 30 days, freedom from primary safety events was 96.4% in AVeVa and 95.0% (Covera™ Vascular Covered Stent) vs. 96.4% (PTA alone) in AVeNEW (P < .0022). Freedom from primary safety events was defined as freedom from an adverse event involving the access circuit resulting in additional intervention, surgery, hospitalization, or death.
Please consult Instructions for Use for product indications for use, contraindications, warnings, precautions, complications, adverse events and detailed safety information.
BD-23522v2
The Covera™ Vascular Covered Stent has been designed to address challenging lesions within in the AV access circuit – including the terminal cephalic arch, the basilic swingpoint segments, and the vein-graft anastomosis.
The Covera™ Vascular Covered Stent delivered effective results in two separate clinical trials, one for patients dialyzing with AV grafts and one for patients dialyzing with AV fistulas, both of which demonstrated the benefits of the stent’s innovative design.1
AVeVA was a prospective, non-randomized, single arm, multi-center study of the Covera™ Vascular Covered Stent used to treat stenoses at the anastomosis of an arteriovenous graft and outflow vein. 110 patients were treated with the Covera™ Vascular Covered Stent at 14 investigational sites in the US
The AVeVA Clinical Study demonstrated that the Covera™ Vascular Covered Stent is effective in the treatment of stenoses at the vein-graft anastomosis of patients dialyzing with an AV graft.
| Study Design | Prospective, Non-Randomized, Multi-Center, Single-Arm |
| Objective | To assess the safety and effectiveness of the Covera™ Vascular Covered Stent for the treatment of stenotic lesions at the graft-vein anastomosis of hemodialysis patients dialyzing with an AV graft |
| Status | 24-month follow-up completed |
| Number of Patients/Sites | 110 patients were treated with the Covera™ Vascular Covered Stent at 14 investigational sites in the US |
| Primary Effectiveness Endpoint | Target Lesion Primary Patency (TLPP) - 6 months |
| Primary Safety Endpoint | Freedom from an adverse event involving the access circuit resulting in additional intervention, surgery, hospitalization, or death through 30 days |
| Follow-Up | 30 & 90 days; 6, 12, 18 & 24 months |
6-Month Target Lesion Primary Patency (TLPP) After Treatment of AV Graft Anastomotic Stenoses with BD Stent Grafts


This chart is for educational purposes only and not for comparison. Differences in study design may impact results. Reference full manuscripts for complete study design details.
In the AVeVA Clinical Study, the Covera™ Vascular Covered Stent was studied in a challenging patient cohort.
| Study Design | Prospective, Multi-Center, Randomized, Concurrently-Controlled |
| Objective | To assess the safety and effectiveness of the Covera™ Vascular Covered Stent for the treatment of stenotic lesions in the upper extremity venous outflow of the AV access circuit of hemodialysis patients dialyzing with an AV fistula |
| Status | 24-month follow-up completed |
| Number of Patients/Sites | 280 randomized subjects in 24 investigational sites (US, EU, & ANZ) |
| Primary Effectiveness Endpoint | Target Lesion Primary Patency (TLPP) - 6 months |
| Primary Safety Endpoint | Freedom from any serious protocol-defined safety event(s) involving the AV access circuit through 30 days |
| Follow-Up | At hospital discharge, 30 & 90 days; 6, 12, 18 & 24 months |
In the AVeNEW Clinical Study, the Covera™ Vascular Covered Stent was used in the treatment of a challenging patient population with difficult lesion characteristics.
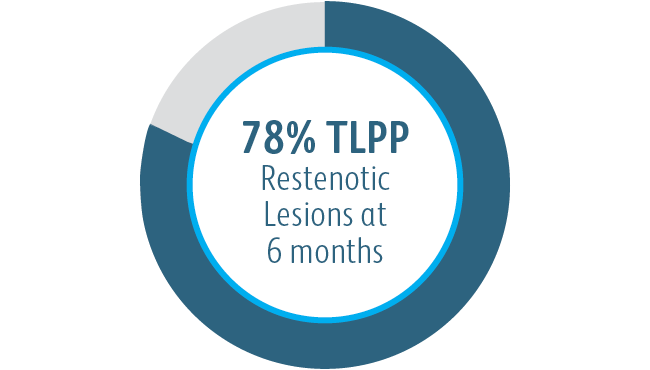
The Covera™ Vascular Covered Stent was superior to the PTA control at 6 & 12 months with respect to TLPP for treatment of stenoses in the venous outflow of patients dialyzing with an arteriovenous fistula.

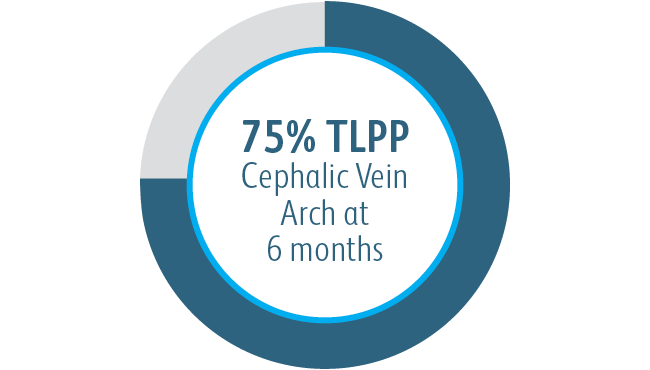
All subgroups showed benefit at 6 months
In all target lesion location subgroups analyzed, the Covera™ Vascular Covered Stent demonstrated greater target lesion primary patency compared to PTA alone, including those treated at the cephalic vein arch.

AVeNEW clinical study additional endpoints
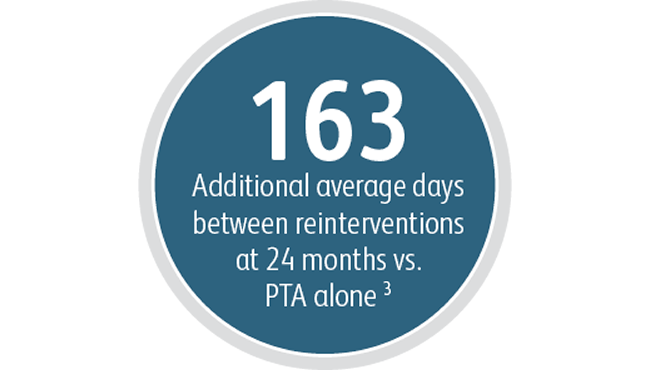
Beyond the benefits in target lesion primary patency, the Covera™ Vascular Covered Stent demonstrated a high degree of Acute Technical Success and extended the average time between interventions at the target lesion compared to PTA alone.
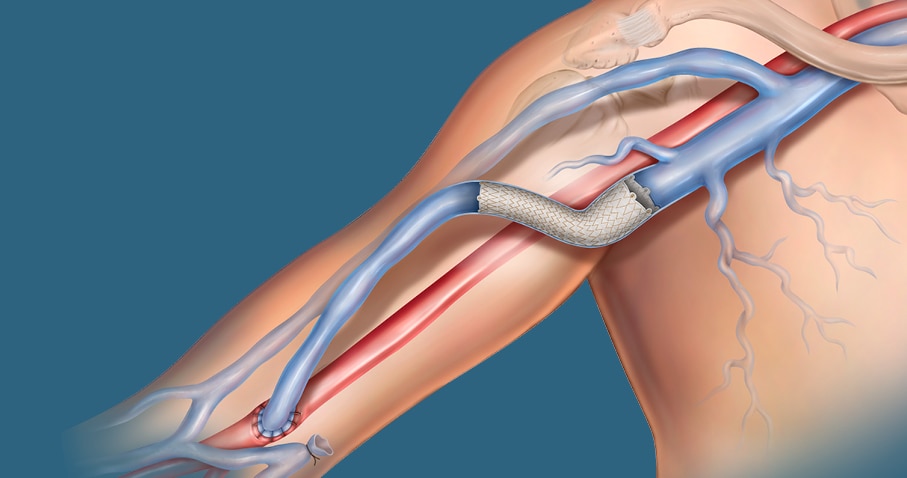
In the AVeNEW clinical study, 77 patients with stenoses in the cephalic vein arch were treated with the
Covera™ Vascular Covered Stent.

This case example demonstrates the baseline angiography showing vessel narrowing and the acute technical success with restoration of the vessel and conformability of the covered stent.
* Haskal ZJ, Trerotola S, Dolmatch B, et al. Stent graft versus balloon angioplasty for failing dialysis-access grafts. N Engl J Med. 2010 Feb 11;362(6):494-503.
** Haskal ZJ, Saad TF, Hoggard JG, et al. Prospective, randomized, concurrently-controlled study of a stent graft versus balloon angioplasty for treatment of arteriovenous access graft stenosis: 2-year results of the RENOVA study. J Vasc Interv Radiol. 2016 Aug;27(8):1105-1114.e3.
***In U.S. as of Nov. 2022
1 Dolmatch B, Waheed U, Balamuthusamy S, Hoggard J, Settlage R; AVeVA Trial Investigators. Prospective, multicenter clinical study of the Covera Vascular Covered Stent in the treatment of stenosis at the graft-vein anastomosis of dysfunctional hemodialysis access grafts. J Vasc Interv Radiol. 2022;33(5):479-488.e3. doi:10.1016/j. jvir.2022.02.008. AVeNEW Clinical Studies data on file. At 6 months in AVeVA, target lesion primary patency (TLPP) was 70.3% (proportional analysis). At 6 months in AVeNEW, TLPP was 78.7% for Covera™ Vascular Covered Stent vs. 47.9% for PTA alone, P < .001. 130 of the 142 (91.5%) subjects randomized to the Covera™ Vascular Stent group and 123 of the 138 (89.1%) randomized to PTA completed their 6-month follow-up. TLPP defined as the interval following the index intervention until the next clinically-driven reintervention at or adjacent to the original treatment site or until the extremity was abandoned for permanent access. In AVeNEW, TLPP at 6 Months – Subgroup Analysis is provided as observational data without P values. In AVeNEW, patients who received the Covera™ Vascular Covered Stent had 103 reinterventions involving a new lesion compared to 72 reinterventions in the PTA only group at 24 months. At 30 days, freedom from primary safety events was 96.4% in AVeVa and 95.0% (Covera™ Vascular Covered Stent) vs. 96.4% (PTA alone) in AVeNEW (P < .0022). Freedom from primary safety events was defined as freedom from an adverse event involving the access circuit resulting in additional intervention, surgery, hospitalization, or death.
2 Acute Technical Success was defined as successful deployment, based on the operator’s opinion, of the implant to the intended location assessed at the time of the index procedure. AVeNEW Clinical Study. Data on File. Bard Peripheral Vascular Inc., Tempe, AZ.
3 Index of Patency Function – Target Lesion (IPF-T) is defined as the time from the index study procedure to study completion or complete access abandonment divided by the number of visits for a reintervention performed at the target lesion in order to maintain vascular access for hemodialysis. Mean IPF-T of 380.40 days with Covera™ Vascular Covered Stent vs. 217.57 days with PTA alone at 24 months. AVeNEW Clinical Study. Data on File. Bard Peripheral Vascular Inc., Tempe, AZ.
Please consult Instructions for Use for product indications for use, contraindications, warnings, precautions, complications, adverse events and detailed safety information.
BD-23522v2
Literature
BD's collection of literature on industry and on our offerings gives you information you can use to continue striving for excellence.
Learn more
Events
BD supports the healthcare industry with market-leading products and services that aim to improve care while lowering costs. We host and take part in events that excel in advancing the world of health™.
Learn more
true
Covera™ Vascular Covered Stent
Safety and Risk Information
Indication for Use
The Covera™ Vascular Covered Stent is indicated for use in hemodialysis patients for the treatment of stenoses in the venous outflow of an arterio-venous (AV) fistula and at the venous anastomosis of an ePTFE or other synthetic AV graft.
Contraindications
There are no known contraindications for the Covera™ Vascular Covered Stent.
Warnings
This device should be used only by physicians who are familiar with the complications, side effects, and hazards commonly associated with dialysis access shunt revisions and endovascular procedures. • DO NOT expose the covered stent to temperatures higher than 500 °F (260 °C). ePTFE decomposes at elevated temperatures, producing highly toxic decomposition byproducts. • DO NOT use the device if packaging / pouch is damaged. • The Covera™ Vascular Covered Stent device is supplied STERILE and is intended for SINGLE USE ONLY. DO NOT RESTERILIZE AND/OR REUSE this device. • DO NOT use in patients with uncorrectable coagulation disorders. • DO NOT use in patients with bacteremia or septicaemia and/or evidence of fistula or graft infection. • DO NOT use in patients that cannot be adequately premedicated and have a known allergy or sensitivity to contrast media. • DO NOT use in patients with known hypersensitivity to nickel-titanium or tantalum. • DO NOT use in an immature fistula or in patients whose AV Access grafts have been implanted less than 30 days. • DO NOT use the device in patients where full expansion of an appropriately sized PTA balloon catheter could not be achieved during pre-dilation with an angioplasty balloon. • Placing a covered stent across a vessel side branch may impede blood flow and hinder or prevent future procedures. • Covered stent placement beyond the ostium of the cephalic vein into the axillary/subclavian vein may hinder or prevent future access. • DO NOT place a flared covered stent with the flared end in a straight vessel segment since this may lead to flow turbulences. The flared end is not intended to provide additional device fixation.
Precautions
Prior to covered stent implantation, read the instructions for use and refer to the sizing table contained therein. Careful attention should be paid to ensure the device is appropriately sized to the vessel diameter, taking into account any change in the vessel diameter that may have resulted from previous interventions. For an AV graft access, utilize the graft diameter as the reference vessel and for an AV fistula access, utilize the inflow vein diameter as the reference vessel. • The appropriate length device should be selected so that the stent graft extends beyond the stenosis into at least 5 mm of the non-diseased fistula or graft towards the arterial inflow and into the non-diseased vein approximately 5 mm beyond the stenosis. • The delivery system is not intended for any use other than covered stent deployment. • The covered stent (implant) cannot be repositioned after total or partial deployment. • Once partially or fully deployed, the covered stent cannot be retracted or remounted onto the delivery system. Device removal after deployment can only be done with a surgical approach. • If unusual resistance is met during covered stent system introduction, the system should be removed and another covered stent system should be used. • DO NOT introduce, manipulate or remove the delivery system without an appropriately sized guidewire in place and without fluoroscopic guidance. • DO NOT kink or use a kinked delivery system. • During covered stent release DO NOT hold the 30 cm long distal catheter assembly segment as it must be free to move and slide into the white stability sheath. • Careful attention by the operator is warranted to mitigate the potential for distal migration of the covered stent during deployment. • Post dilation of the covered stent must be performed using an appropriately sized PTA balloon catheter to avoid damage to the covered stent. The covered stent cannot be post dilated beyond its labelled diameter. The flared distal end does not require post dilation. • The effect of placing the device across an aneurysm or a pseudo-aneurysm has not been evaluated. • The effect of using the device in central veins has not been evaluated. • The effect of placing the device across a previously placed bare metal stent has not been evaluated. • The effect of placing the device across the antecubital fossa has not been evaluated. • The effect of using the device in pediatrics has not been evaluated. • The effect of using the device across the anastomosis of an AV fistula has not been evaluated. • Vessel angulation was not measured as part of the clinical study, as such limitations in covered stent angulation are unknown. • DO NOT cannulate the covered stent. Notify the patient that the covered stent should not be directly cannulated for hemodialysis and that applying pressure to the implant area should be avoided. • The device has not been tested for use in an overlapped condition with a bare metal stent or covered stent. • Higher deployment force may be encountered with longer length covered stents. • The device has not been tested for tracking and deployment around an AV loop graft. • Serious complications, such as migration to the heart or lungs, may occur post-discharge when covered stents have not been appropriately sized. • Stent graft dislodgement may occur during removal of the delivery system; therefore, careful attention should be paid during this portion of the procedure to prevent such occurrences.
Potential Complications and Adverse Events
Complications and Adverse Events associated with the use of the Covera™ Vascular Covered Stent may include the usual complications associated with endovascular stent and covered stent placement and dialysis shunt revisions. Potential complications may include, but are not limited to: New lesions in the access circuit requiring reintervention; thrombotic occlusion; restenosis of the target lesion requiring reintervention; pseudoaneurysm; vessel rupture; dissection; extravasation; perforation; pain; infection; hemorrhage; hematoma; arm or hand edema; steal syndrome; congestive heart failure; cerebrovascular accident; allergic reaction; rash; reaction to contrast; fever; sepsis; prolonged bleeding, ventricular fibrillation; face or neck edema; bleeding at access site; numbness; venous spasm; hemoptysis and death.
Please consult product labels and package inserts for indications, contraindications, hazards, warnings, cautions, and information for use.
BD, the BD logo, and Covera are trademarks of Becton, Dickinson and Company or its affiliates. © 2022 BD. All Rights Reserved. Becton, Dickinson and Company | www.bd.com |1 800 321 4254 | 1625 W. 3rd Street, Tempe, AZ 85281
BD-79752
true